| PANDEMIC ALERT LEVEL |
| 123456 |
| Tracking the next pandemic: Avian Flu Talk |
Oxygen Treatment |
Post Reply 
|
| Author | |
ezmeralda 
Valued Member 
Joined: February 10 2006 Status: Offline Points: 3 |
 Post Options Post Options
") Thanks(0) Thanks(0)
 Quote Reply Quote Reply
 Topic: Oxygen Treatment Topic: Oxygen TreatmentPosted: February 10 2006 at 12:36pm |
|
Does one need a doctor's prescription to buy oxygen at the medical supply places? I see some old people moving around with their oxygen tanks. It seems like it might be a good idea if you've gotten so sick with the flu that you're at the point of suffocation in your own lung fluid that having pure oxygen might help. Although from what I understand there's a proper way to administer it. Does anybody here know the do's and don'ts of breathing pure oxygen? Like maybe someone here is a nurse.
|
|
 |
|
|
Guests
Guest Group 
|
Post Options
Thanks(0)
Quote Reply
Posted: February 10 2006 at 4:50pm |
|
Originally posted by Fla_Medic: This is my first post on this board, Please be gentle. Edited by SophiaZoe |
|
|
|
|
Guests
Guest Group
|
Post Options
Thanks(0)
Quote Reply
Posted: February 10 2006 at 5:21pm |
|
Ezmeralda, a little primer on Oxygen. It's a good subject to discuss.
First, Oxygen is a drug. And like all drugs, when administered properly, it can have a benificial effect. When improperly used, it can have serious reprocussions. Anytime a patient is in respiratory difficulty, administering oxygen is probably going to help. Patients with COPD (chronic obstructive Pulmonary Disease) can not tolorate high does of oxygen, and can actually overdose and stop breathing. This condition usually resolves it'self when the patient's CO2 blood levels return to normal. But to be safe, limit oxygen to only 4 liters/min. Obtaining oxygen requires an Rx in most, if not all, states. Small bottles of oxygen will only last a couple of hours (depends on the flow rate). Oxygen concentrators can run a long time, but do require electricity. Oxygen equipment is not cheap, and is usually rented. Assuming you can get you hands on oxygen, you need to be aware that oxygen, while not flamable, with serve as a catalyst and even a small spark can start a fire. The combustion can be so rapid, that it will seem more like an explosion than a fire. So no smoking in and around oxygen equipment! Administering oxygen is fairly easy. Most of the time, a nasal canula works best. Masks can be claustrophobic for some patients. They slip into the nostrils and are held in place by wrapping them around the ears. Masks provide a higher concentration of oxygen, and can be used if a patient will tolorate them. However, a flu patient, who is coughing a lot, may have difficulty using one. For most patients, a flow rate of 4-6 liters is about right. If a patient does well on 4 liters, you can turn it down a bit, titrate for effect. Oxygen is very dry, and the addition of an in-line humidifier is often used. You can tell if the oxygen is helping by the patient's color, and if the patient is struggling less for air. Now for the realities. Oxygen, while helpful, isn't going to do much for a patient in ARDS. If the lungs are filled with fluids, there will be little or no oxygen exchange. Of more potential value, and easier to obtain, is a suction machine. The ability to suction secretions from the patient's airway will probably do more for an ARDS patient (assuming anything will help), than simply pushing oxygen. Medical supply houses sell them, and some are battery operated. A simple suction machine could also be built using a small air compressor, some suction tube, and a collection bottle. Would make an easy weekend project for a handyman. Bottom line, if you have Oxygen, use it when a patient is cyanotic (looks like a smurf). For those who are only in mild respiratory distress, having them take a `hit' off of an oxygen tank every few minutes might suffice. It might allow you to stretch the limited supply on hand. Oxygen can also be used for suspected heart attacks. Chest pain is often a sign of poor oxygenation of the heart muscle. Raising the patient's oxygen blood level can help prevent cardiac damage. Hope some of this helps.  |
|
|
|
|
Guests
Guest Group
|
Post Options
Thanks(0)
Quote Reply
Posted: February 10 2006 at 5:30pm |
|
FM... would you consider elaborating on the suction....? SZ |
|
|
|
|
Guests
Guest Group
|
Post Options
Thanks(0)
Quote Reply
Posted: February 10 2006 at 5:49pm |
 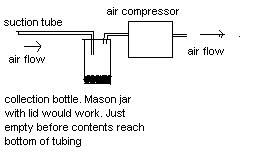 Okay, this is a quickie example of how to build a suction machine.  Tubing can be bought at any hardware store. Thin, preferably clear, and flexible. Be sure to remove any sharp edges from the end that you will use in the patient's throat. A bic lighter, gently applied, can soften the plastic. Place a collection jar inline between the suction tubing and the aircompressor. A mason jar with two holes in the lid will work. The patient tube should extend further into the jar that the exhaust tube (going to the compressor). The exhaust tube goes to the INTAKE of the aircompressor. If you cut a small notch into the top of the suction tube, about 18 inches from the end, you can use your thumb to adjust the suction rate. Simply close off the hole to suction. Wear Gloves! Obviously, you will need a small compressor. A big one will be too powerful. I'd be willing to bet one of those air compressors designed to blow up air mattresses could be used, and they only run about $10. Fitting the tube to the intake might take some `engineering', but I'm sure something could be rigged. Hope this helps!
Edited by Fla_Medic |
|
|
|
|
Guests
Guest Group
|
Post Options
Thanks(0)
Quote Reply
Posted: February 11 2006 at 8:49am |
|
In the near future I�ll be posting stratgeies, and identifying therputic entities, to help survive a Cytokine Storm following exposure to Bird Flu / H5N1. |
|
|
|
|
Guests
Guest Group
|
Post Options
Thanks(0)
Quote Reply
Posted: February 11 2006 at 8:55am |
|
Rick, if you have a handle on CS I, personally, will drop and worship at your feet, if you help guide us through the labyrinth. SZ |
|
|
|
|
Rocky
V.I.P. Member 

Joined: January 07 2006 Location: United States Status: Offline Points: 219 |
Post Options
Thanks(0)
Quote Reply
Posted: February 13 2006 at 10:55am |
|
Will be on the lookout for your posting. Will it be at this site? Rocky
QUOTE=Rick] In the near future I�ll be posting stratgeies, and identifying therputic entities, to help survive a Cytokine Storm following exposure to Bird Flu / H5N1. [/QUOTE] |
|
 Rocky Rocky |
|
|
|
|
Post Reply
|
|
 Tweet
Tweet
|
| Forum Jump | Forum Permissions You cannot post new topics in this forum You cannot reply to topics in this forum You cannot delete your posts in this forum You cannot edit your posts in this forum You cannot create polls in this forum You can vote in polls in this forum |








 Topic Options
Topic Options